Mitomycin C
- admin
-
 Offline
Offline
- Posts: 1163
- Thank you received: 153
A little bit of science for the weekend 
Those of you who, like me, without being fully informed, had Mitomycin C applied before surface ablation treatment (lasek/PRK) will no doubt find this 2012 paper as scary as I do!
'What We Don’t Know
“We’re doing surface ablations in patients who are 21 years old. We really don’t know what effect this will have when they’re 70,” Dr. Wilson said. Forty years from now, will ophthalmologists be seeing stromal melting or unhealthy epithelium in these eyes? “I’ve never seen anything to suggest that it’s going to be a problem, but my understanding of corneal biology makes me continue to worry about it.”*
Dr. Majmudar agreed that long-term safety remains a concern. Nonetheless, he noted, “We’ve seen enough patients treated over the past 15 years that if problems were going to occur, we would likely have seen some hint of them by now.”**
While it’s reassuring to see patients who are doing well many years later, Dr. Hofmeister stressed that MMC is used off label. “It’s an area of extreme controversy,” she said. “We’re taking healthy eyes that see well [and treating them]. Above all, we don’t want to harm people.”'***
www.aao.org/eyenet/article/15-years-of-m...tion-tips-techniques
* (i) I was 57 when I had laser eye surgery!
(ii) If Dr Wilson is worried, then those of us who've had MMC sure as hell should be!
**Liar - they've seen more than 'some hint' of problems!
***I repeat, liar! They harm people as a matter of course, then treat us like lab rats, to be discussed, dissected, 'let's test this on the next one...'
And of course laughed at by sickos like Parag Majmudar and his colleagues - the surgeon who 'entertained' colleagues by mocking suicidal patients in his disgusting performance at an ASCRS convention in 2009, YouTube video posted here 15 March.
As for laser or lens replacement surgery age suitability, this should be of interest if you haven't previously seen it!
PS: Like so many ex-Optical Express surgeons, no mention of his previous employer here... www.communityhealthservices.co.uk/ourcli...tonio-uceda-montanes
Or here... optilase.com/our-surgeons/
Wayne Crewe-Brown coincidentally OE's choice of medicolegal defence expert!
Those of you who, like me, without being fully informed, had Mitomycin C applied before surface ablation treatment (lasek/PRK) will no doubt find this 2012 paper as scary as I do!
'What We Don’t Know
“We’re doing surface ablations in patients who are 21 years old. We really don’t know what effect this will have when they’re 70,” Dr. Wilson said. Forty years from now, will ophthalmologists be seeing stromal melting or unhealthy epithelium in these eyes? “I’ve never seen anything to suggest that it’s going to be a problem, but my understanding of corneal biology makes me continue to worry about it.”*
Dr. Majmudar agreed that long-term safety remains a concern. Nonetheless, he noted, “We’ve seen enough patients treated over the past 15 years that if problems were going to occur, we would likely have seen some hint of them by now.”**
While it’s reassuring to see patients who are doing well many years later, Dr. Hofmeister stressed that MMC is used off label. “It’s an area of extreme controversy,” she said. “We’re taking healthy eyes that see well [and treating them]. Above all, we don’t want to harm people.”'***
www.aao.org/eyenet/article/15-years-of-m...tion-tips-techniques
* (i) I was 57 when I had laser eye surgery!
(ii) If Dr Wilson is worried, then those of us who've had MMC sure as hell should be!
**Liar - they've seen more than 'some hint' of problems!
***I repeat, liar! They harm people as a matter of course, then treat us like lab rats, to be discussed, dissected, 'let's test this on the next one...'
And of course laughed at by sickos like Parag Majmudar and his colleagues - the surgeon who 'entertained' colleagues by mocking suicidal patients in his disgusting performance at an ASCRS convention in 2009, YouTube video posted here 15 March.
As for laser or lens replacement surgery age suitability, this should be of interest if you haven't previously seen it!
PS: Like so many ex-Optical Express surgeons, no mention of his previous employer here... www.communityhealthservices.co.uk/ourcli...tonio-uceda-montanes
Or here... optilase.com/our-surgeons/
Wayne Crewe-Brown coincidentally OE's choice of medicolegal defence expert!
Last Edit:18 May 2019 15:19
by admin
Reply to admin
Note: BBcode and smileys are still usable.
- admin
-
Offline
- Posts: 1163
- Thank you received: 153
Most of you won't have heard of Mitomycin C (MMC), a drug generally used in cancer treatment
en.wikipedia.org/wiki/Mitomycin_C
www.cochrane.org/CD002897/EYES_mitomycin-c-for-glaucoma-surgery
Although unlicensed for use in laser eye surgery, there are few clinics/surgeons that do not use MMC for lasek/PRK. But unfortunately, we guinea pigs are not always advised of the facts, and even when we are they're presented in such a casual way that we don’t worry because the doctor knows best - or so we all believed once upon a time!
MMC was not mentioned or discussed with me at any point prior to the moment when Optimax surgeon Wilbert Hoe thrust the four page MMC consent form in front of me minutes before surgery - allowing me no time to research it - telling me nothing more than it was to stop post op haze, and to sign it.
Given the way it was presented to me I accepted that it was no big deal, so I signed the MMC Consent form without time to read.
In fact, it was a massive big deal!
And had I been fully informed pre surgery, and given an opportunity to research the drug, then I wouldn’t be talking to you now, because there is no way I would have agreed to having MMC administered to my eyes.
It was only post surgery, realising that I had serious problems, that I read the MMC Consent, which states that, ‘Optimax does not endorse the use of Mitomycin-C in it’s [sic] clinics and recommends the non-use of Mitomycin-C in all cases where there is an alternative option (e.g. waiting). Most haze will clear with time. Medical practitioners treating with this drug do so determined by their own clinical judgement and take responsibility for any after effects due to its use experienced by individual and properly informed patients.’
If 'most haze will clear with time', then I should have been given the option to refuse. And I challenge anyone in the industry who dares argue that I was given a choice to contact me, and I'll be happy to debate this publicly!
And if Optimax don't endorse its use, then who provides the MMC? Does the doctor walk around with it in his bag, or is it ordered from Optimax’ pharma supplier? In which case this surely negates their claim that they do ‘not endorse the use of Mitomycin-C'!
'If ethanol [alcohol] use during LASEK produces similar effects as MMC, MMC will not be as necessary as in conventional PRK’
pdfs.semanticscholar.org/a986/7a865ce98c...35f5e6e93c610445.pdf
Alcohol was also used on my eyes during lasek...
'Even though ophthalmologists have 15 years of experience with Mitomycin C (MMC) to treat and prevent corneal haze following surface ablation, questions still abound regarding its optimal use and long-term safety.’
www.aao.org/eyenet/article/15-years-of-m...tion-tips-techniques
Reading through my Optimax MMC consent form earlier,I was horrified to read a paragraph that included this from US ophthalmologist Dr Randy Epstein, suggesting that, ‘the appropriateness of using Mitomycin-C prophylactically is likely to be more controversial when performing myopic PRK or LASEK in eye which are poor LASIK candidates because of thin corneas or large pupils.’
I had thin corneas and large pupils, though the latter was never addressed pre surgery.
I asked a number of surgeons for copies of their MMC consent forms, one of which included the following info, 'MMC is very potent and potentially toxic under certain circumstances. Complications are very rare and some eye-related complications that have been reported following the use of MMC (for other conditions – NOT Laser eye surgery) include: conjunctival injection (redness of the eye), permanent stem cell deficiency, corneal or scleral thinning or perforation, corneal de-compensation requiring corneal transplantation, cataract, and retinal vascular occlusion. The complications listed above were seen following various types of eye surgeries and possibly with incorrect dosage and concentration of MMC.’
Regular readers will know that I suffered two retinal vein occlusions last year, which caused a macular oedema. This was treated with monthly injections until the swelling reduced, and just as I was optimistically expecting to be told no more injections, another oedema occurred!
Whilst no retinal surgeon could tell me whether the occlusions have anything to do with my laser surgery, other than being stress related, I will always argue that any problems I suffer with my eyes, without a definitive known cause, are a result of laser. And I was therefore not too surprised to read that MMC has been linked to occlusions after eye surgery. The caveat ‘NOT laser’ is as convincing to me as the industry’s claim that laser eye surgery does not cause dry eyes ar MGD.
Only retinal surgeons at Moorfields have details of my branch retinal vein occlusions (BRVO). In my opinion therefore, the possibility of a connection to laser surgery cannot be so easily dismissed by refractive surgeons, and until data is collected detailing the numbers who’ve similarly suffered occlusions after laser, their argument is as valid as mine, possibly less so.
I have read many research papers written by (refractive) surgeons comparing studies of lasik v lasek etc, but little time is spent researching the post op problems we all suffer! Because if this were honestly investigated, without skewed data to suit their own agenda (£$) and the truth told, the numbers of people undergoing laser/RLE would plummet, and thousands of surgeons worldwide would be scrabbling for new jobs!
And when I read research papers referring to the effect of laser eye surgery/MMC on countless rabbits’ eyes I want to cry, because the pain these animals must suffer is inconceivable. At least I knew the cause of the intense and relentless pain I suffered for three days post op, and understand why I still suffer pain and can’t see very well, and that no amount of carrots will ever help me see in the dark again, but what those poor animals must suffer horrifies me.
NB: I do not intend to enter debate concerning animal research.
While this unregulated corrupt and incestuous industry experiment on our eyes, boast about successes at their conferences and discuss more ways to f*ck up our eyes, it is entirely at the expense of our healthy eyes and quality of life.
And I am unimpressed by the industry’s reliance on meta-analytics, not least because without true statistics they’re flawed and unreliable. I deal with the end results, very real people left irreparably damaged, all for the profit of surgeons (and businessmen) who manage to sleep at night, no matter how many people they’ve hurt.
Doctors are expected to heal people, not harm them!
en.wikipedia.org/wiki/Mitomycin_C
www.cochrane.org/CD002897/EYES_mitomycin-c-for-glaucoma-surgery
Although unlicensed for use in laser eye surgery, there are few clinics/surgeons that do not use MMC for lasek/PRK. But unfortunately, we guinea pigs are not always advised of the facts, and even when we are they're presented in such a casual way that we don’t worry because the doctor knows best - or so we all believed once upon a time!
MMC was not mentioned or discussed with me at any point prior to the moment when Optimax surgeon Wilbert Hoe thrust the four page MMC consent form in front of me minutes before surgery - allowing me no time to research it - telling me nothing more than it was to stop post op haze, and to sign it.
Given the way it was presented to me I accepted that it was no big deal, so I signed the MMC Consent form without time to read.
In fact, it was a massive big deal!
And had I been fully informed pre surgery, and given an opportunity to research the drug, then I wouldn’t be talking to you now, because there is no way I would have agreed to having MMC administered to my eyes.
It was only post surgery, realising that I had serious problems, that I read the MMC Consent, which states that, ‘Optimax does not endorse the use of Mitomycin-C in it’s [sic] clinics and recommends the non-use of Mitomycin-C in all cases where there is an alternative option (e.g. waiting). Most haze will clear with time. Medical practitioners treating with this drug do so determined by their own clinical judgement and take responsibility for any after effects due to its use experienced by individual and properly informed patients.’
If 'most haze will clear with time', then I should have been given the option to refuse. And I challenge anyone in the industry who dares argue that I was given a choice to contact me, and I'll be happy to debate this publicly!
And if Optimax don't endorse its use, then who provides the MMC? Does the doctor walk around with it in his bag, or is it ordered from Optimax’ pharma supplier? In which case this surely negates their claim that they do ‘not endorse the use of Mitomycin-C'!
'If ethanol [alcohol] use during LASEK produces similar effects as MMC, MMC will not be as necessary as in conventional PRK’
pdfs.semanticscholar.org/a986/7a865ce98c...35f5e6e93c610445.pdf
Alcohol was also used on my eyes during lasek...
'Even though ophthalmologists have 15 years of experience with Mitomycin C (MMC) to treat and prevent corneal haze following surface ablation, questions still abound regarding its optimal use and long-term safety.’
www.aao.org/eyenet/article/15-years-of-m...tion-tips-techniques
Reading through my Optimax MMC consent form earlier,I was horrified to read a paragraph that included this from US ophthalmologist Dr Randy Epstein, suggesting that, ‘the appropriateness of using Mitomycin-C prophylactically is likely to be more controversial when performing myopic PRK or LASEK in eye which are poor LASIK candidates because of thin corneas or large pupils.’
I had thin corneas and large pupils, though the latter was never addressed pre surgery.
I asked a number of surgeons for copies of their MMC consent forms, one of which included the following info, 'MMC is very potent and potentially toxic under certain circumstances. Complications are very rare and some eye-related complications that have been reported following the use of MMC (for other conditions – NOT Laser eye surgery) include: conjunctival injection (redness of the eye), permanent stem cell deficiency, corneal or scleral thinning or perforation, corneal de-compensation requiring corneal transplantation, cataract, and retinal vascular occlusion. The complications listed above were seen following various types of eye surgeries and possibly with incorrect dosage and concentration of MMC.’
Regular readers will know that I suffered two retinal vein occlusions last year, which caused a macular oedema. This was treated with monthly injections until the swelling reduced, and just as I was optimistically expecting to be told no more injections, another oedema occurred!
Whilst no retinal surgeon could tell me whether the occlusions have anything to do with my laser surgery, other than being stress related, I will always argue that any problems I suffer with my eyes, without a definitive known cause, are a result of laser. And I was therefore not too surprised to read that MMC has been linked to occlusions after eye surgery. The caveat ‘NOT laser’ is as convincing to me as the industry’s claim that laser eye surgery does not cause dry eyes ar MGD.
Only retinal surgeons at Moorfields have details of my branch retinal vein occlusions (BRVO). In my opinion therefore, the possibility of a connection to laser surgery cannot be so easily dismissed by refractive surgeons, and until data is collected detailing the numbers who’ve similarly suffered occlusions after laser, their argument is as valid as mine, possibly less so.
I have read many research papers written by (refractive) surgeons comparing studies of lasik v lasek etc, but little time is spent researching the post op problems we all suffer! Because if this were honestly investigated, without skewed data to suit their own agenda (£$) and the truth told, the numbers of people undergoing laser/RLE would plummet, and thousands of surgeons worldwide would be scrabbling for new jobs!
And when I read research papers referring to the effect of laser eye surgery/MMC on countless rabbits’ eyes I want to cry, because the pain these animals must suffer is inconceivable. At least I knew the cause of the intense and relentless pain I suffered for three days post op, and understand why I still suffer pain and can’t see very well, and that no amount of carrots will ever help me see in the dark again, but what those poor animals must suffer horrifies me.
NB: I do not intend to enter debate concerning animal research.
While this unregulated corrupt and incestuous industry experiment on our eyes, boast about successes at their conferences and discuss more ways to f*ck up our eyes, it is entirely at the expense of our healthy eyes and quality of life.
And I am unimpressed by the industry’s reliance on meta-analytics, not least because without true statistics they’re flawed and unreliable. I deal with the end results, very real people left irreparably damaged, all for the profit of surgeons (and businessmen) who manage to sleep at night, no matter how many people they’ve hurt.
Doctors are expected to heal people, not harm them!
Last Edit:22 Sep 2018 14:16
by admin
Reply to admin
Note: BBcode and smileys are still usable.
- Fiver
Animal Lover wrote: Can someone tell me how the f*ck a rabbit read a Snellen chart??
A talking rabbit to boot :pinch:
Last Edit:25 Oct 2014 17:15
by Fiver
Reply to Fiver
Note: BBcode and smileys are still usable.
- Animal Lover
Can someone tell me how the f*ck a rabbit read a Snellen chart??
www.pubfacts.com/author/Kazakos+Dimitris+C
"Similarly, eyes in groups 3 and 4 underwent PRK to correct -10 D in a 6-mm optical zone, while sponges soaked with 0.02% MMC were applied on the exposed corneal stroma for 60 and 120 seconds, respectively."
Kazakos Dimitris C
I had Lasek (same pain as PRK) and MMC and it was the worst pain I could imagine for more than 3 days!!
Poor rabbits
www.pubfacts.com/author/Kazakos+Dimitris+C
"Similarly, eyes in groups 3 and 4 underwent PRK to correct -10 D in a 6-mm optical zone, while sponges soaked with 0.02% MMC were applied on the exposed corneal stroma for 60 and 120 seconds, respectively."
Kazakos Dimitris C
I had Lasek (same pain as PRK) and MMC and it was the worst pain I could imagine for more than 3 days!!
Poor rabbits
Last Edit:25 Oct 2014 16:21
by Animal Lover
Reply to Animal Lover
Note: BBcode and smileys are still usable.
- admin
-
Offline
- Posts: 1163
- Thank you received: 153
As I sit here suffering with painful and itchy dry eyes, I thought I'd refresh this topic - not so easily done to my eyes!
"Photorefractive keratectomy with mitomycin C treatment could induce or exacerbate dry eye."
This is true for Lasek, the (mis)treatment I had.
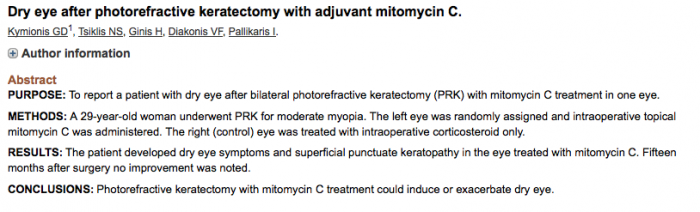
www.ncbi.nlm.nih.gov/pubmed/16722493
"Photorefractive keratectomy with mitomycin C treatment could induce or exacerbate dry eye."
This is true for Lasek, the (mis)treatment I had.
www.ncbi.nlm.nih.gov/pubmed/16722493
Last Edit:17 Aug 2014 13:52
by admin
Reply to admin
Note: BBcode and smileys are still usable.
- Monet
-
 Offline
Offline
- Posts: 1
- Thank you received: 0
I recently requested my medical notes after deciding to go for a second opinion on OE's offer of an intraocular lens implant to my extremely poor left eye, following LASIK and LASEK procedures on both eyes.
Just scanned my medical notes for the enhancement procedure, and yes, the notes say: "due to accomodation on wavescan, best to enhance EK standard (Bilateral) (not WF). MMC required." The requirement for MMC was not explained to me at the time.
What really bugged me is the blasé way they apply exclamation marks all over the notes.
e.g. "Symptoms: no change... cl's only removed when arrived for appointment!" I'm soooo sorry. Was it a serious problem? If so, why did you not tell me, reschedule the examination, explaining that the tests would be compromised? But you didn't, did you? You just went ahead, in your own breezy kinda way.
"R excellent, L bit blurry ... Not sure why vision affected - similar Rx!" Yeah. Wowzers Scooby, Isn't it just like, a TOTAL mystery?!
"PX will go to OE Manchester for refraction check - advised cyclo refraction then!!!!!" Five exclamation marks. Jeez, whatever cyclo refraction means, it must be funny. Or should that read 'serious'?
OE, this isn't jolly japes. These are customers experiencing serious problems due to your mistakes. The apparent concern expressed to the patient in the examination room doesn't seem to transfer to the computer screen when your examiners swing around in their cheapo swivel chair to start typing in their hilarious notes. Professional decorum should be applied to note taking as well.
Take note. Go on, and try not to add an exclamation mark this time.
Just scanned my medical notes for the enhancement procedure, and yes, the notes say: "due to accomodation on wavescan, best to enhance EK standard (Bilateral) (not WF). MMC required." The requirement for MMC was not explained to me at the time.
What really bugged me is the blasé way they apply exclamation marks all over the notes.
e.g. "Symptoms: no change... cl's only removed when arrived for appointment!" I'm soooo sorry. Was it a serious problem? If so, why did you not tell me, reschedule the examination, explaining that the tests would be compromised? But you didn't, did you? You just went ahead, in your own breezy kinda way.
"R excellent, L bit blurry ... Not sure why vision affected - similar Rx!" Yeah. Wowzers Scooby, Isn't it just like, a TOTAL mystery?!
"PX will go to OE Manchester for refraction check - advised cyclo refraction then!!!!!" Five exclamation marks. Jeez, whatever cyclo refraction means, it must be funny. Or should that read 'serious'?
OE, this isn't jolly japes. These are customers experiencing serious problems due to your mistakes. The apparent concern expressed to the patient in the examination room doesn't seem to transfer to the computer screen when your examiners swing around in their cheapo swivel chair to start typing in their hilarious notes. Professional decorum should be applied to note taking as well.
Take note. Go on, and try not to add an exclamation mark this time.
Last Edit:26 Nov 2013 23:24
by Monet
Reply to Monet
Note: BBcode and smileys are still usable.
- Bowman's layer permanently removed
Bowman's membrane/layer is permanently removed during refractive surface ablation (lasek, prk,...). Bowman's membrane is the second layers in cornea after epithelium. Epithelium and Bowman's membrane is removed during refractive surface ablation, but the only membrane/layer that regenerate is the epithelium (the top cornea layer). This could lead to serious eye problems in the future. Patients aren't informed about this problem because it doesn't sell surgeries. Surgery without a true informed consent is against the law.
www.ophthobook.com/questions/question-na...a-and-their-function
"Bowmans Layer: A tough layer of basement membrane right under the epithelium. This layer is tough, and keeps the cornea from swelling forward … which means when the cornea swells, it must do so backwards into the anterior chamber."
quizlet.com/7688340/print/
"Bowman's Membrane: function, and what occurs if damaged?
-protects against infection, and strengthens the cornea
-it can't regenerate, so if it becomes damaged, scarring can occur"
www.ophthobook.com/questions/question-na...a-and-their-function
"Bowmans Layer: A tough layer of basement membrane right under the epithelium. This layer is tough, and keeps the cornea from swelling forward … which means when the cornea swells, it must do so backwards into the anterior chamber."
quizlet.com/7688340/print/
"Bowman's Membrane: function, and what occurs if damaged?
-protects against infection, and strengthens the cornea
-it can't regenerate, so if it becomes damaged, scarring can occur"
by Bowman's layer permanently removed
Reply to Bowman's layer permanently removed
Note: BBcode and smileys are still usable.
- Pandora
-
 Offline
Offline
- Posts: 20
- Thank you received: 1
Quotes:
Francesco Carones:
"The major criticism in the use of MMC after laser refractive surgery refers to the potential side effects and complications associated with its long-term cytostatic action on tissues when applied in a topical fashion on the corneal stroma. Several researchers have reported corneoscleral melt after MMC application after pterygium excision. Also, the long-term integrity of the endothelial layer is supposed to be at risk."
Steven E Wilson:
"I encourage you to use the same technology to look at patients who are having mitomycin prophylactic treatment for prevention of haze; probably 90 percent of refractive surgeons are using mitomycin without any long-term data as to the effect. It is clear the reason mitomycin works so well is that it eliminates 100 percent of all corneal cells in about 20 percent of the anterior cornea. Similar to your concerns, I think they are even magnified in those patients because data after six months in the animal model shows that none of those cells have returned. What happens in the future since we have limited experience with these types of patients? In 10 to 20 years, are we going to see anterior corneal necrosis or other problems? Your type of study could give us more data about that in humans."
Robert Doyle Stulting:
"Pathology in this case suggests cell loss and abnormalities of keratocytes, leading us to wonder whether defective keratocyte metabolism could make ectasia more likely and to wonder whether Mitomycin C might increase the long-term risk of ectasia"
Steve Schallhorn:
"A single application of low-dose mitomycin C (MMC) is highly effective in treating and preventing haze and scarring, said Steven C. Schallhorn, M.D., director of refractive surgery, U.S. Navy, San Diego. That’s according to a review of the current scientific literature on MMC. There also has been no reported serious complication of MMC. However, he said, ophthalmologists still don’t understand the dosage implications of MMC, he said. The longest follow up with MMC has only been three years."
www.centrolaser.net/products.asp?prod=73&cat=0&hierarchy=
www.ncbi.nlm.nih.gov/pubmed/16722493
www.ncbi.nlm.nih.gov/pmc/articles/PMC2694026/
www.ncbi.nlm.nih.gov/pubmed/14508259
Francesco Carones:
"The major criticism in the use of MMC after laser refractive surgery refers to the potential side effects and complications associated with its long-term cytostatic action on tissues when applied in a topical fashion on the corneal stroma. Several researchers have reported corneoscleral melt after MMC application after pterygium excision. Also, the long-term integrity of the endothelial layer is supposed to be at risk."
Steven E Wilson:
"I encourage you to use the same technology to look at patients who are having mitomycin prophylactic treatment for prevention of haze; probably 90 percent of refractive surgeons are using mitomycin without any long-term data as to the effect. It is clear the reason mitomycin works so well is that it eliminates 100 percent of all corneal cells in about 20 percent of the anterior cornea. Similar to your concerns, I think they are even magnified in those patients because data after six months in the animal model shows that none of those cells have returned. What happens in the future since we have limited experience with these types of patients? In 10 to 20 years, are we going to see anterior corneal necrosis or other problems? Your type of study could give us more data about that in humans."
Robert Doyle Stulting:
"Pathology in this case suggests cell loss and abnormalities of keratocytes, leading us to wonder whether defective keratocyte metabolism could make ectasia more likely and to wonder whether Mitomycin C might increase the long-term risk of ectasia"
Steve Schallhorn:
"A single application of low-dose mitomycin C (MMC) is highly effective in treating and preventing haze and scarring, said Steven C. Schallhorn, M.D., director of refractive surgery, U.S. Navy, San Diego. That’s according to a review of the current scientific literature on MMC. There also has been no reported serious complication of MMC. However, he said, ophthalmologists still don’t understand the dosage implications of MMC, he said. The longest follow up with MMC has only been three years."
www.centrolaser.net/products.asp?prod=73&cat=0&hierarchy=
www.ncbi.nlm.nih.gov/pubmed/16722493
www.ncbi.nlm.nih.gov/pmc/articles/PMC2694026/
www.ncbi.nlm.nih.gov/pubmed/14508259
Last Edit:23 Nov 2013 13:50
by Pandora
Reply to Pandora
Note: BBcode and smileys are still usable.
- Mr Starburst
-
 Offline
Offline
- Posts: 97
- Thank you received: 12
Replied by Mr Starburst on topic Physical violation re Mitomycin C (MMC)
Posted 23 Nov 2013 12:21 #9
I have seen information that the LASEK procedure it's generally used in permanently destroys the Bowman's layer/membrane of the cornea.
If this is correct, all those who've had this operation without being informed of the above prior to surgery have been denied informed consent, effectively prevented from reaching a truly informed decision and therefore the surgeon must be adjudged to have committed physical assault!
If this is correct, all those who've had this operation without being informed of the above prior to surgery have been denied informed consent, effectively prevented from reaching a truly informed decision and therefore the surgeon must be adjudged to have committed physical assault!
Last Edit:23 Nov 2013 13:40
by Mr Starburst
Reply to Mr Starburst
Note: BBcode and smileys are still usable.
- Caro
It is a physical violation to perform any procedure on a person without their fully informed consent and can leave them as traumatised as if they'd been raped (and possibly like me left with permanent, life changing injuries).
Last Edit:22 Nov 2013 12:51
by Caro
Reply to Caro
Note: BBcode and smileys are still usable.
Moderators: admin